Hip Labral Tear
Hip impingement is a condition that usually affects young active individuals where there is a collision between the femoral head-neck junction and the rim of the acetabulum during normal functional hip movements. This is often the cause of labral tears, as it is not common for the labrum to tear in the absence of a shape problem in the hip joint. Commonly the shape problems are due to a cam lesion or pincer lesion. Labral tears may also occur due to hip dysplasia, a traumatic injury, or arthritis.
Any sport may contribute to hip impingement and labral tear however the typical sports include dancing, power lifting, paddling, martial arts, cycling, rugby, AFL, running, hockey and soccer.
Dr Agolley is a hip surgeon on the Gold Coast who has a special interest in Hip impingement and labral tears. He will discuss the diagnosis and cause of your hip impingement and labral tear with you.
What is a Cam lesion of the hip?
A cam lesion of the hip occurs when there is increased bone at the junction of the femoral head and neck. During normal functional hip flexion, the bump rubs and impinges on the inside of the acetabulum and labrum. Repetitive impingement over years causes delamination of the joint cartilage and splits the labrum from the bony rim. Hip impingement is something that develops during adolescence, and grinds away over time. Often this continues un-noticed and without any symptoms, where studies have identified up to 15% of the population to have asymptomatic cam lesions. However, the damage progresses slowly over time, and in those that become symptomatic, something changes where they begin to perceive pain. It is likely that the labrum splits and pain fibres are aggravated, or due to cartilage delamination, the subchondral bone is exposed to excessive pressure.
With progressive repetitive injury, there is ongoing damage in your hip joint leading to early osteoarthritis.
Dr Agolley uses hip arthroscopy to address the damaged cartilage and correct the shape of the hip joint to minimise ongoing damage the hip joint from the impinging bone.
What is a Pincer lesion of the hip?
A pincer lesion of the hip occurs where the bony rim of the acetabulum (socket) extends in the front of the hip abnormally, limiting the normal functional flexion of the hip joint. The front of the femoral neck collides (impinges) with the front of the socket rim. Dr Agolley performs hip arthroscopy, to address the rim, and alleviate the impinging bone. Occasionally, hip arthroscopy is not the solution to the impinging bone, and other hip preservation procedures are more appropriate which Dr Agolley will discuss with you.
When Should I have Surgery?
Pain from hip impingement and labral tear is usually sharp or a dull ache at the front of the hip in the groin area, and occasionally refers to the buttock region or down the thigh or the knee. Impingement pain is aggravated by deep hip flexion activities where your knee is brought to your chest e.g. squatting or sitting for long periods of time, or standing from a seated position. The pain may have come on gradually over time, or after a sudden incident like a deep squat or jump. It is common for many patients with hip impingement to have previously had another diagnosis such as adductor strain, groin strain or osteitis pubis, and not make progress with rehabilitation often having an aggravation of the groin pain due to deep hip flexion exercises. As your hip damage becomes more advanced, the pain is present not just during or after sport, but present all the time. Simple tasks such as walking and jogging become troublesome, impeding your ability to work and take part in enjoyable activities in life.
What investigations will be required?
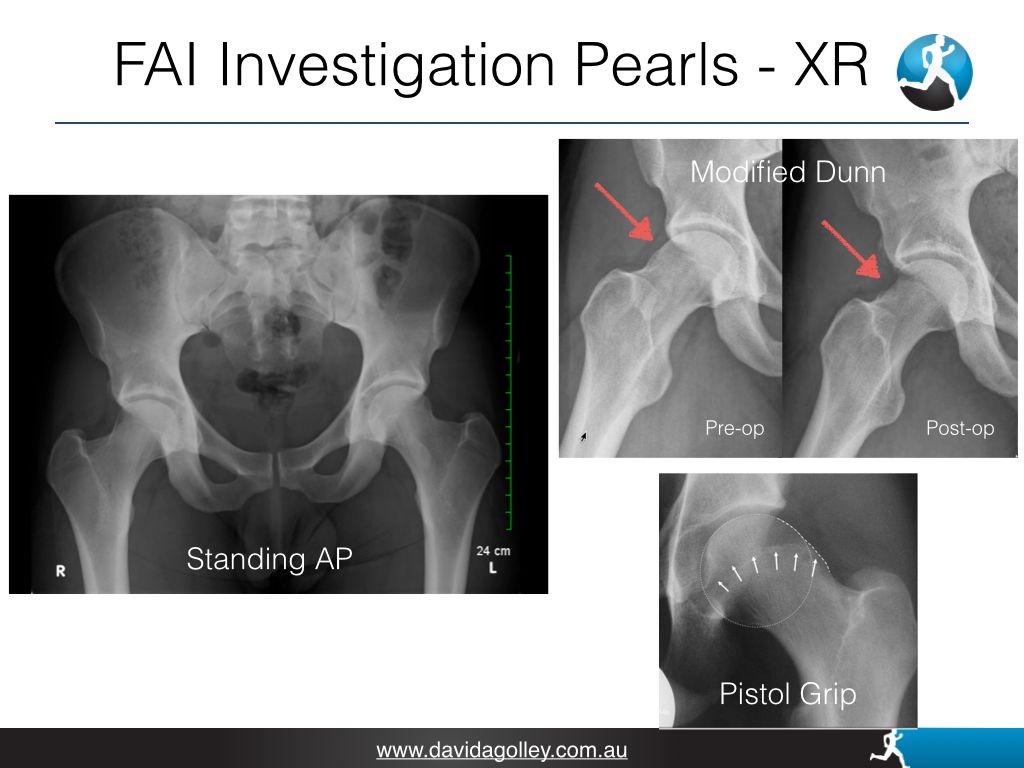
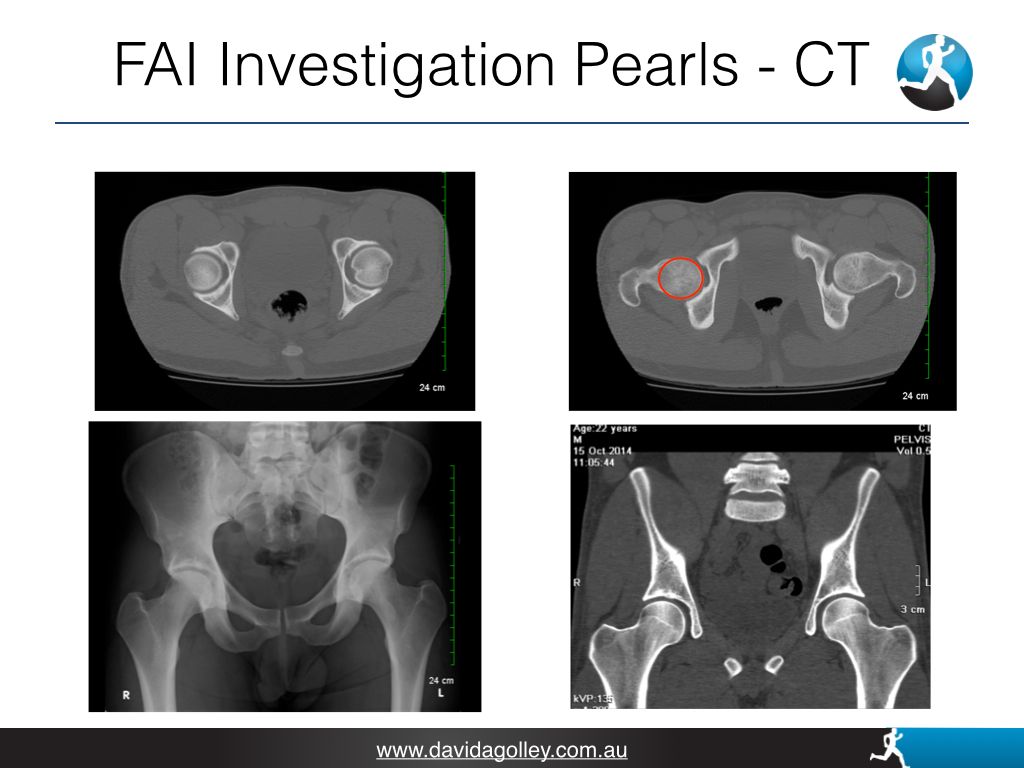
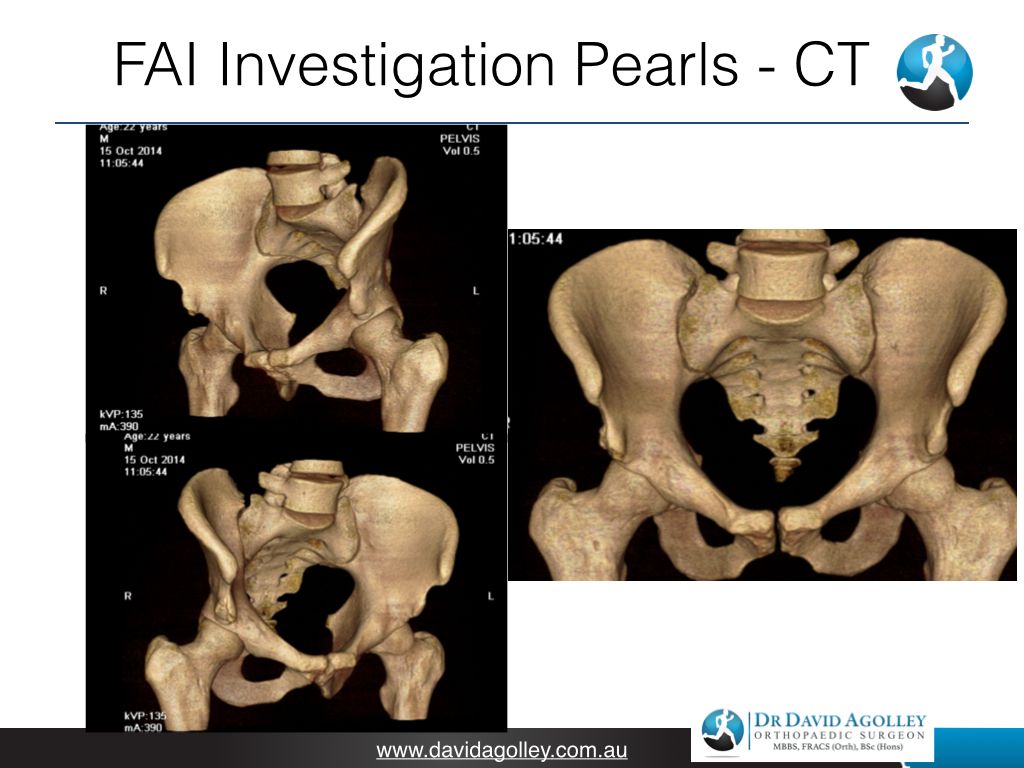
Plain x-rays of your pelvis taken in a standing weight bearing position and modified Dunn view of both hips is essential. An MRI or CT scan is usually not required for initial consultation. Dr Agolley will request further scans if deemed necessary.
When should I have surgery?
Non-surgical treatments involve limiting deep hip flexion, low impact activity (swimming and cycling with a high seat), keeping your weight down, changing your activity or occupation if feasible, physiotherapy for core strengthening but to avoid deep hip flexion exercises, and taking pain medication can be helpful.
If the non-surgical treatment is not successful, hip arthroscopy may be recommended. Some hip pathology is not amenable to hip arthroscopy, and Dr Agolley will discuss the options with you.
More Information
For more information, see the American Academy or Orthopaedic Surgeon website.